Micro-Randomized Trials: An Experimental Design for Developing Just-in-Time Adaptive Interventions 요약
논문
Micro-Randomized Trials: An Experimental Design for Developing Just-in-Time Adaptive Interventions Predrag Klasnja1, Eric B. Hekler2, Saul Shiffman3, Audrey Boruvka1, Daniel Almirall1, Ambuj Tewari1, and Susan A. Murphy1 1University of Michigan 2Arizona State University 3University of Pittsburgh Database: APA PsycArticles Health Psychology, 34(Suppl), 1220–1228.
Introduction
모바일 기기와 센서 기술 발전으로 mHealth interventions를 사용자의 자연스러운 생활 맥락에서 제공하는 것이 가능해짐.
사용자가 필요할 때 요청하는 pull 방식 interventions는 취약한 상태나 기회 상태에 있을 때 사용자의 인식과 동기에 의존함. -> 센서, self-report, algorithm을 활용해 개입 시점을 판단하는 push 방식 interventions가 중요해짐.
JITAI는 언제, 어디서, 어떤 intervention component를 제공할지에 대한 명시적 decision rules를 갖는 intervention으로 큰 잠재력 가짐.
기술은 빠르게 발전했지만, 이를 뒷받침할 experimental methodology와 behavioral theory 부족.
기존 theory는 인간 행동의 temporal dynamics를 충분히 세밀하게 설명하지 못해 decision rule 설계에 한계가 있음.
-> 제안: MRT
Current methods for intervention optimization
Randomized Controlled Trials(RCTs): intervention package 전체의 평균 효과는 평가 가능. 개별 intervention components의 효과, delivery timing, time-varying moderation은 평가하기 어려움. secondary analysis에서 time-varying effects를 다룰 경우 causal confounding 위험이 큼. 이것이 평균적으로 효과가 있는가?
Single-Case Experimental Designs(SCEDs): within-subject comparison이 가능해 효율적, decision point와 effect moderation을 체계적으로 다루기 어려움. 이 사람한테 이 intervention 효과 있는가?
Factorial designs and Multiphase Optimization Strategy(MOST): 각 intervention component의 main effect와 interaction은 평가 가능, 언제 intervention을 제공해야 하는지는 다루지 못함. time-varying factors에 의한 moderation 분석 불가능. 여러 intervention components 중 어떤 것이 효과가 있는가? 언제 써야하는지는 모르는 것.
기존 방법들은 JITAI optimization에 필요한 핵심 질문을 해결하지 못함.
Micro-randomized trial design
각 decision point마다 intervention option 무작위로 할당. 여러 intervention components를 동시에 randomize할 수 있어 sequential factorial design의 성격. 한 participant당 수백-수천 번의 randomization이 발생할 수 있음. 반복 randomization을 통해 causal effects의 시간적 변화를 추정할 수 있음. between-subject contrasts와 within-subject contrasts를 모두 활용해 높은 efficiency.
An example of a micro-randomized trial
HeartSteps는 physical activity를 촉진하기 위한 mHealth intervention.
두 가지 주요 intervention components: 1) daily activity planning(언제 어디서 어떻게 걸을지 미리 생각), 2) contextually-relevant activity suggestions(알림 보낼지 말지). daily planning은 매일 저녁 randomization, activity suggestions는 하루 5개 decision point에서 randomization, suggestion delivery 여부와 suggestion type이 단계적으로 randomization.
6주 동안 개인당 daily planning 42회, activity suggestions 210회의 data 생성.
Distal, proximal, and lagged outcomes
distal outcome은 intervention 전체의 궁극적인 목표.
proximal outcome: 특정 intervention component가 delivery된 직후 의도된 효과, distal outcome의 mediator 역할을 할 수 있음. proximal outcome이 반드시 distal outcome의 단기 버전일 필요는 없음.
lagged effects: 즉각적 반응이 아닌 이후 시점에서 나타나는 효과. lagged effects를 이해하는 것은 low-burden JITAI 설계에 중요.
Randomization and participant availability
모든 decision point에서 intervention delivery가 항상 적절한 것은 아님.
intervention이 부적절한 경우 participant는 unavailable로 간주.
randomization은 participant가 available한 경우에만 이루어짐.
availability는 effect estimation에서 반드시 고려되어야 함.
Research questions for micro-randomized trials
1) 각 intervention component의 proximal effects와 lagged effects는 무엇인가? 2) 이러한 effects는 시간에 따라 어떻게 변화하는가? 3) 어떤 time-invariant 또는 time-varying factors가 effects를 moderation하는가?
이 질문들에 대한 답은 JITAI decision rules 설계로 이어짐.
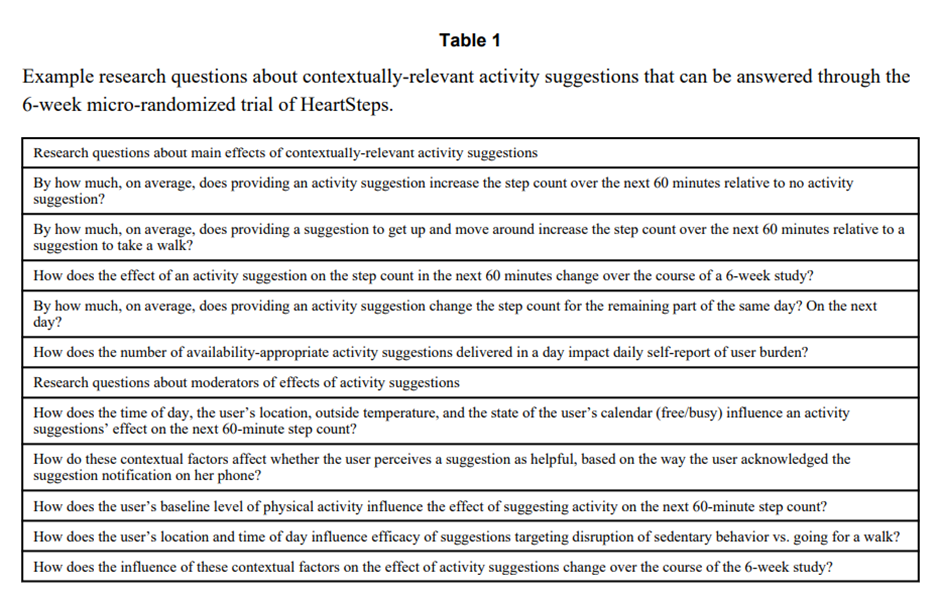
위 세 질문들에 대한 구체적인 질문들.
Data-analytic issues in micro-randomized trials
MRTs는 intensive longitudinal data 생성.
multilevel models (MLM)과 generalized estimating equations (GEE)을 활용할 수 있음.
bias와 participant availability가 핵심 analytic issues임.
Analyses for assessing proximal effects
primary analyses는 proximal main effects를 탐지하는 데 초점.
main effect는 다른 components와 interactions를 평균한 효과.
MLM 또는 GEE로 proximal effects를 추정.
time terms를 포함해 time-varying effects를 추정할 수 있음.
covariates는 intervention의 영향을 받지 않는 변수만 포함해야 함.
Level 1: Proximal Step Count is modeled by Time, Intervention and Weather

i번째 participant의 t번째 날 proximal outcome(다음날 step count)이 시간, weather, intervention, 그리고 intervention x time 상호작용으로 어떻게 결정되는지를 나타내는 Level 1 model.
Y_it: i번째 participant의 t시점 proximal outcome -> 다음 날 step count
π_0i: i번째 participant의 기본 평균 step count 수준(intercept)
π_1i t: 시간에 따른 선형 변화 -> intervention과 무관하게 시간이 지나면서 step count가 증가, 감소하는 경향
π_2i t^2: 시간에 따른 quadratic 변화 -> 초반 증가 후 정체, 감소 후 회복 같은 패턴 (This simple model uses a quadratic function for day to model a time-varying effect of evening planning.)
A_it: intervention option -> 1: evening planning occurred, 0: did not occur
W_it: weather: 1: good, 0: bad
B_i: baseline average daily step count
π_3i W_it: weather effect -> 날씨가 좋을 때와 나쁠 때 step count 차이, intervention과 무관한 순수 맥락 효과
π_4i A_it: evening planning intervention의 proximal main effect -> planning을 한 날과 안한 날 다음 날 step count 평균 차이, 시간 평균된 효과
π_5i A_it t: intervention effect가 시간에 따라 선형적으로 변하는지
π_6i A_it t^2: intervention effect의 비선형 시간 변화
ϵ_it: residual -> 컨디션, 측정 오차 등
Level 2: Participant Differences are modeled by Baseline Step Count

각 참가자의 level 1 계수는 baseline step count와 개인차로 나눌 수 있음.
π_ki: i번째 participant의 level 1 계수, k는 level 1에서의 항. -> k=0: intercept, k=1: time(t) … 사람마다 intercept 다르고, time trend, intervention 효과 전부 다름.
β_k0: population-level 평균 계수 -> basline step count가 0인 가상의 사람에서의 평균값, 전체 평균적인 k번째 효과
β_k1 B_i: baseline step count가 level 1 계수에 미치는 영향
δ_ki: baseline step count로도 설명되지 않는 개인 고유의 랜덤 편차 -> 생활 패턴, 성향 등
Participant availability
proximal main effect는 available한 occasions에 대해서만 정의됨.
effect는 intervention x availability interaction으로 추정되어야 함.
available population은 시간에 따라 변할 수 있음.
availability 자체도 secondary analysis의 대상이 될 수 있음.
Analyses of time-varying moderation
context, psychosocial variables 등이 proximal effects를 어떻게 moderation하는지 분석 가능.
intervention x moderator x time interactions로 추정. -> user burden을 최소화하면서 efficacy를 극대화하는 decision rule 설계에 기여함.
Power
MRTs는 매우 efficient한 design. within-subject와 between-subject contrasts를 모두 활용. 소규모 sample size로도 small effect detection 가능.
Micro-randomized trials and theoretical grounding of JITAI design
behavioral theory는 intervention component 설계에는 유용했으나 delivery rule 설계에는 한계가 있음.
implementation details가 user experience와 efficacy에 큰 영향을 미침.
기존 theory는 temporal dynamics를 충분히 설명하지 못함.
MRTs는 theoretical constructs의 time- and context-dependent dynamics를 경험적으로 밝힘.
Implementation considerations for micro-randomized trials
MRT 설계 시 고려해야 할 practical issues를 다룸.
Deciding which components to randomize and how
evidence가 부족하거나 dynamics가 불명확한 components를 randomize함.
여러 implementation alternatives 중 선택을 안내할 수 있음.
randomization rate는 power와 participant burden을 함께 고려해 결정함.
Defining proximal outcomes
일부 components는 proximal outcome 명확.
그렇지 않은 경우 researcher judgment와 feasibility 필요.
직접 측정이 burden을 유발할 경우 passive outcome 선택.
proximal outcome이 mediator인 경우 theoretical justification 필요.
Limitations
MRTs는 push interventions에만 적용 가능.
proximal outcomes를 반복적으로 low-burden 측정할 수 있어야 함.
rare events를 다루는 interventions에는 부적합.
Conclusion
JITAIs는 건강 행동 지원을 크게 향상시킬 잠재력이 있음.
적절한 optimization methods의 부재가 발전을 제한해 왔음.
micro-randomized trials는 이 한계를 극복하기 위한 핵심 methodology.
